
Case 11
Figure 1. Colour fundus photograph of the left eye reveals intraretinal flame-shaped haemorrhages in the left superonasal macula.
Author and Editor: Adrian Fung
A 42-year-old Caucasian female was referred by her optometrist with a 1 week history of mildly reduced vision in her left eye.
Case history
A 42-year-old Caucasian female was referred with a 1 week history of slightly reduced vision in her left eye. She had no significant past ocular or medical history. She did not take the oral contraceptive pill and was a non-smoker.
On examination her visual acuities were right (OD) 6/6 and left (OS) 6/7.5 (no improvement with pinhole). Intraocular pressures were 9mmHg OD and 10mmHg OS. Anterior segment examination was normal with no iris neovascularisation. Posterior segment demonstrated intraretinal flame-shape and blot haemorrhages in the superonasal left macula (Figure 1). There was loss of the foveal reflex and a yellowish discolouration of the fovea suggestive of associated cystoid macular oedema.
What is your diagnosis?
Click to reveal answer
DIAGNOSIS
Left macular branch retinal vein occlusion (BRVO) with associated cystoid macular oedema (CMO).
Additional history, examination and investigations
Spectral-domain optical coherence tomography (OCT) confirmed the clinically suspected cystoid macular oedema (Figure 2). A fundus fluorescein angiogram (FFA) demonstrated the mildly dilated macular vein and angiographic cystoid macular oedema (Figures 3 & 4). There was subtle widening of the intercapillary spaces superonasal to the foveal avascular zone.
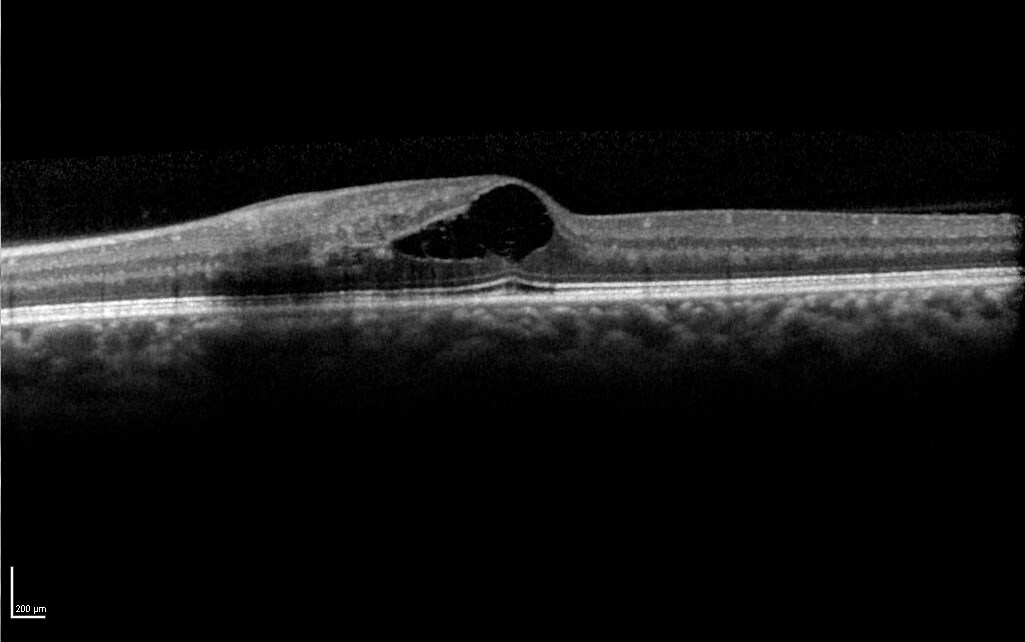
Figure 2. Spectral-domain optical coherence tomography demonstrated cystoid macular oedema. Note the integrity of the foveal photoreceptor layer in particular the ellipsoid zone (IS-OS junction) and external limiting membrane (ELM).
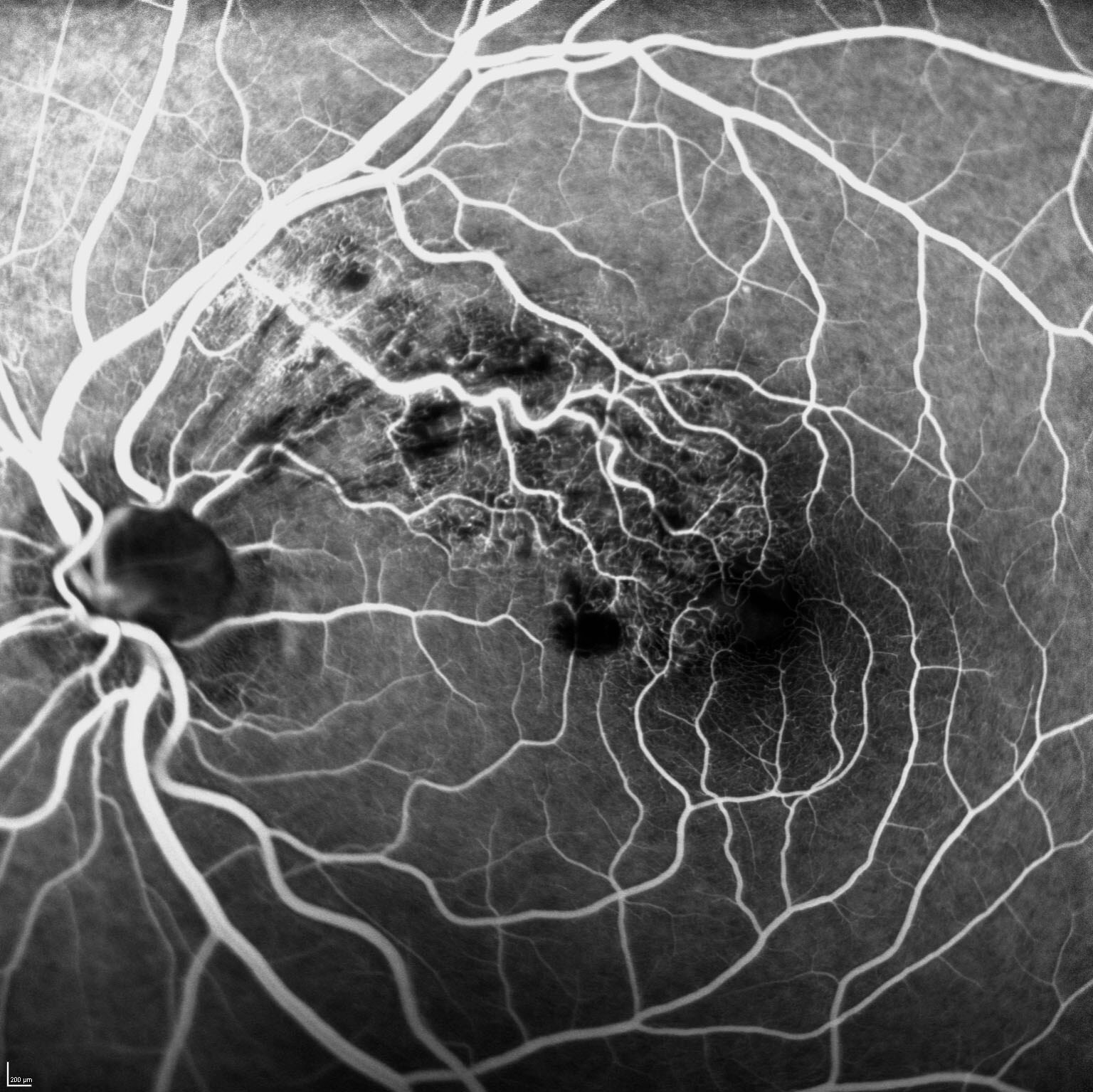
Figure 3. Early-mid phase FFA demonstrates mild dilatation of the occluded macular vein and blocked fluorescence due to haemorrhage. There was subtle widening of the intercapillary spaces superonasal to the foveal avascular zone.
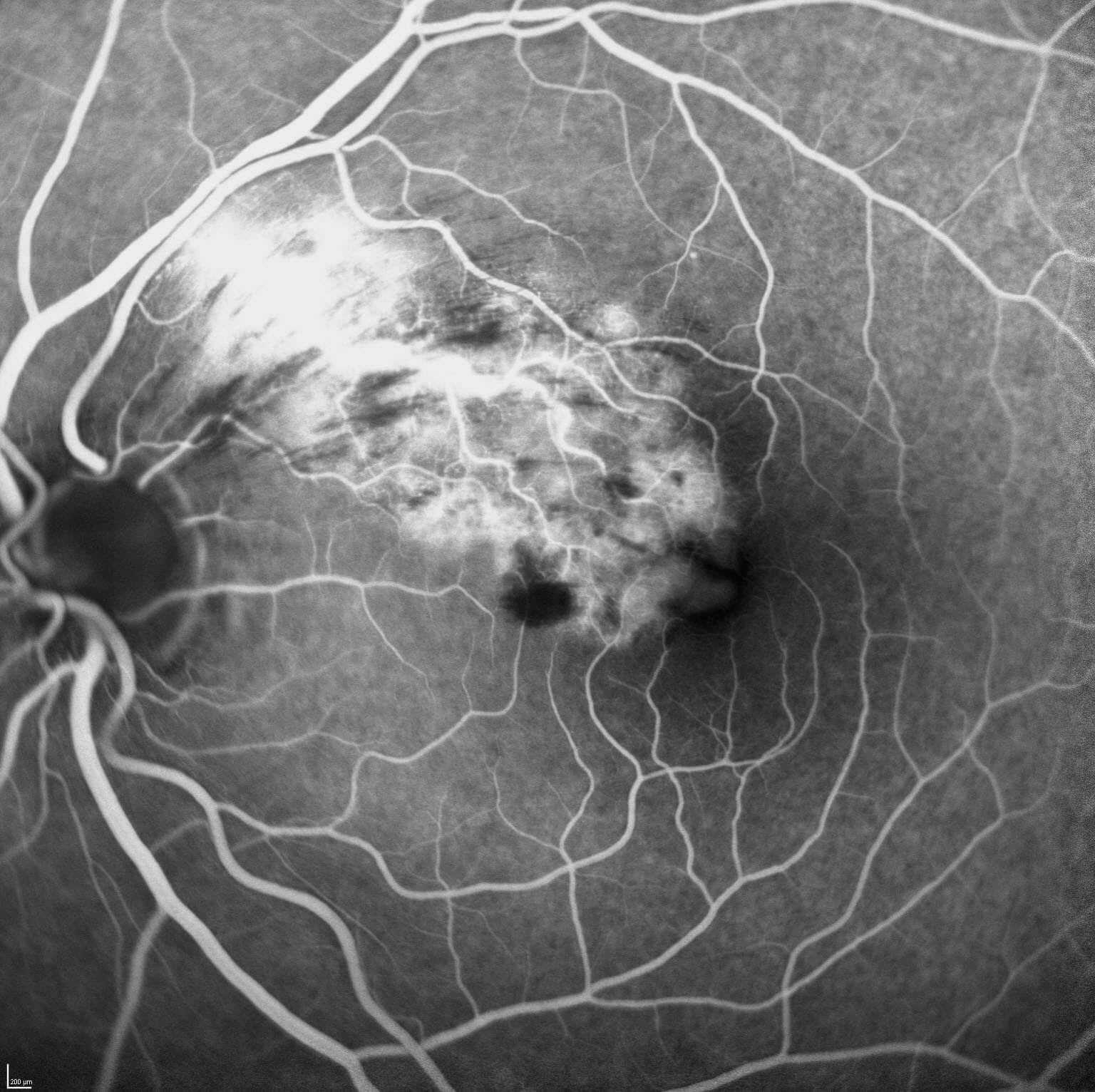
Figure 4. Late phase FFA of the left eye demonstrates leak and angiographic cystoid macular oedema.
Clinical course
The clinical findings and diagnosis were discussed with the patient. As the natural history can include spontaneous resolution of the macular oedema and in light of her relative good visual acuity an initial period of observation was undertaken.
Given her young age further systemic investigations were carried out to identify any underlying risk factors. This included a thrombophilic screen and vascular studies. She was found to be hypertensive (blood pressure 162mmHg/96mmHg) for which she was prescribed anti-hypertensive medications and regular exercise.
At the one month review there was persistent cystoid macular oedema with a mild increase in central retinal thickness. Correspondingly her left visual acuity had dropped to 6/9. After discussing the potential benefits and risks of anti-VEGF treatment an ‘off-label’ intravitreal injection of bevacizumab (Avastin®) 1.25mg in 0.05mL was administered. One month post-injection her left visual acuity had improved to 6/6. OCT images demonstrated a dramatic response with a normal foveal contour and minimal residual intraretinal fluid (Figure 5). In the ensuing months further intravitreal Avastin® injections were required to maintain a ‘dry’ macula. Limited grid laser photocoagulation was applied in an attempt to reduce the number of intravitreal anti-VEGF injections and the associated risks. At 12 months the patient’s macula remained ‘dry’ and left visual acuity measured 6/4.8. In light of possible disc cupping the patient underwent further evaluation including Humphrey visual fields and OCT of the retinal nerve fibre layers. These were normal and the findings were thought to be consistent with physiological cupping.
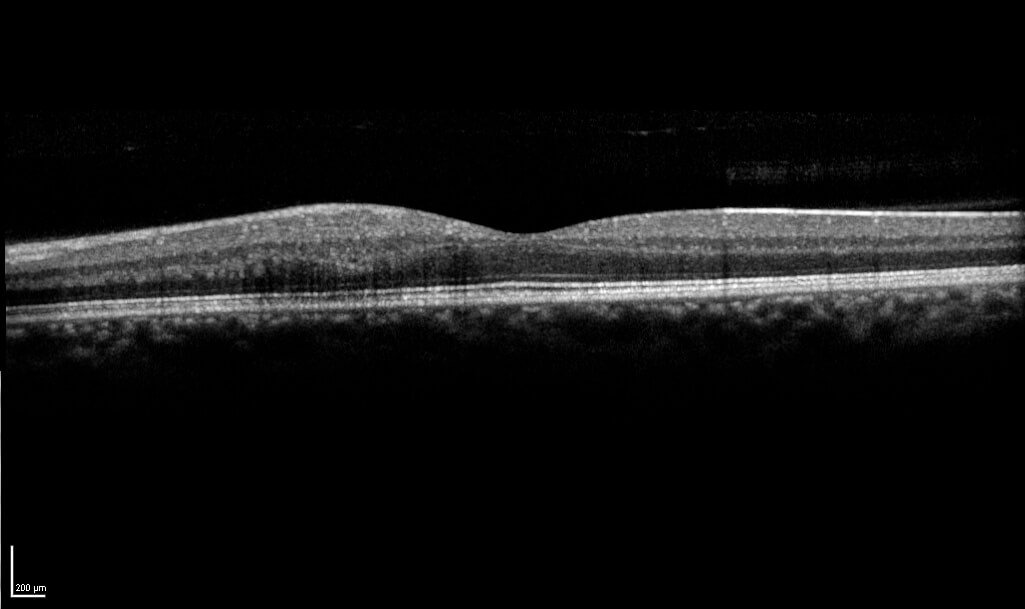
Figure 5. OCT image demonstrating a significant response 1 month after a single intravitreal bevacizumab injection. There is minimal residual intraretinal fluid.
Discussion
Branch retinal vein occlusions (BRVO) are the second most common retinal vascular disorder after diabetic retinopathy and are an important cause of visual loss. The prevalence is approximately 0.6% and it affects both genders equally,(1) most commonly after the age of 60 years(2). Presenting symptoms may include sudden painless loss of vision or a visual field defect. It may also be detected incidentally on routine examination particularly if it involves the nasal retina or distal extra-macular vessels. Vision loss can be due to macular oedema, fovea ischaemia or neovascular complications such as vitreous haemorrhage.
Clinical features include intraretinal haemorrhages in a wedge-shaped distribution corresponding to the drainage of the obstructed vessel. Cotton wool spots are sometime seen. It should be noted whether the occlusion occurs at an arteriovenous crossing site. Signs of predisposing conditions may be present including hypertensive retinopathy (arteriovenous nicking, arteriolar narrowing or opacification/‘copper wiring’). In the acute phase the clinician should look for complications, particularly cystoid macular oedema. Retinal neovascularisation and vitreous haemorrhage typically occur late in the course of the disease. Chronic residual signs include microaneurysms, dilated capillaries, telangeictatic vessels and collateral vessel formation.
Cardiovascular risk factors, particularly hypertension, hyperlipidaemia, diabetes mellitus and smoking are key predisposing factors. This is in keeping with arterial disease and atherosclerosis being the predominant pathogenic mechanism in most cases.(2) In these typical cases the vein occlusions occur at arteriovenous crossing sites at which thick-walled arteries cross and compress thin-walled veins.
When BRVOs occur in young patients or in bilateral cases (particularly with no systemic risk factors) consideration should be given to directed investigations for thrombophilic and vasculitic predispositions. These investigations however often prove negative and the exact role these risk factors play in retinal vein occlusions remain unclear. A recent meta-analysis analysing risk factors in retinal vein occlusions concluded that thrombophilic diseases (specifically factor V Leiden mutation, hyperhomocysteinemia and anticardiolipin antibodies) and vasculitis do increase the risk of retinal vein occlusions.(3) In females the use of an oral contraceptive pill is known to increase the risk. In the case described, undiagnosed hypertension was identified and it could be argued that further screening was not essential. As it turned out the investigations indeed proved negative.
Further evaluation of a patient with a BRVO involves optical coherence tomography (OCT) and fluorescein angiography (FFA). Optical coherence tomography scans allows detection of even mild macular oedema and monitoring of progress with each visit. Continuity of the foveal ellipsoid zone and external limiting membrane has been found to be associated with better visual outcomes (Figure 2).(4) The characteristic FFA finding is that of delayed filling of the obstructed vein. Other retinal vascular features may include capillary non-perfusion, telangiectatic collateral vessels, microaneurysms, retinal neovascularisation and angiographic macular oedema. If there is dense macular haemorrhage the associated blocked fluorescence limits interpretation and the FFA is best delayed. FFA can help differentiate whether reduced visual acuity is secondary to macula oedema or ischaemia.
Understanding the natural history of BRVO associated macular oedema and visual outcomes is fundamental when considering the management options. It needs to be appreciated that in a proportion of patients the macular oedema may spontaneously resolve and it is reasonable to allow an initial period of observation.(5) If however the macular oedema fails to resolve or, as in our case, increases with a further reduction in visual acuity, intervention is appropriate. The treatment options include intravitreal anti-VEGF injections, macular grid laser and/or steroids.(6,7,8) Anti-VEGF treatment is largely accepted as the first line treatment. Recently trials and further studies will clarify if combination therapy might decrease treatment burden whilst maintaining optimal visual outcomes.(9,10) Scatter laser photocoagulation is indicated when retinal neovascularization occurs to prevent vitreous haemorrhage.(6)
TAKE HOME POINTS
- Branch retinal vein occlusion may cause vision loss due to macular oedema or ischaemia (acutely) or retinal neovascularization with vitreous haemorrhage (in the later stages).
- Classic risk factors include hypertension, hyperlipidaemia, diabetes mellitus and smoking.
- In young patients an underlying predisposing condition such as thrombophilia or vasculitis should be considered.
- On optical coherence tomography the continuity of the ellipsoid zone and external limiting membrane has prognostic significance.
First line treatment for branch retinal vein occlusion associated macular oedema is intravitreal anti-VEGF injections.
REFERENCES